
[ad_1]
Highlights of History
- No State has seen a decline in its rate of diabetes since 2008-2009
- Obesity has climbed in 34 states during the same period, while it decreased
- Increase in diabetes related to increased interstate obesity
WASHINGTON, DC – The percentage of adults diagnosed with diabetes at one point in their lives has grown in 18 US states in less than ten years, according to a comparison of data from the 2016-2017 Gallup-Sharecare Wellbeing Index compared to 2008-2009 data. Diabetes rates did not decline in any state during the same period.
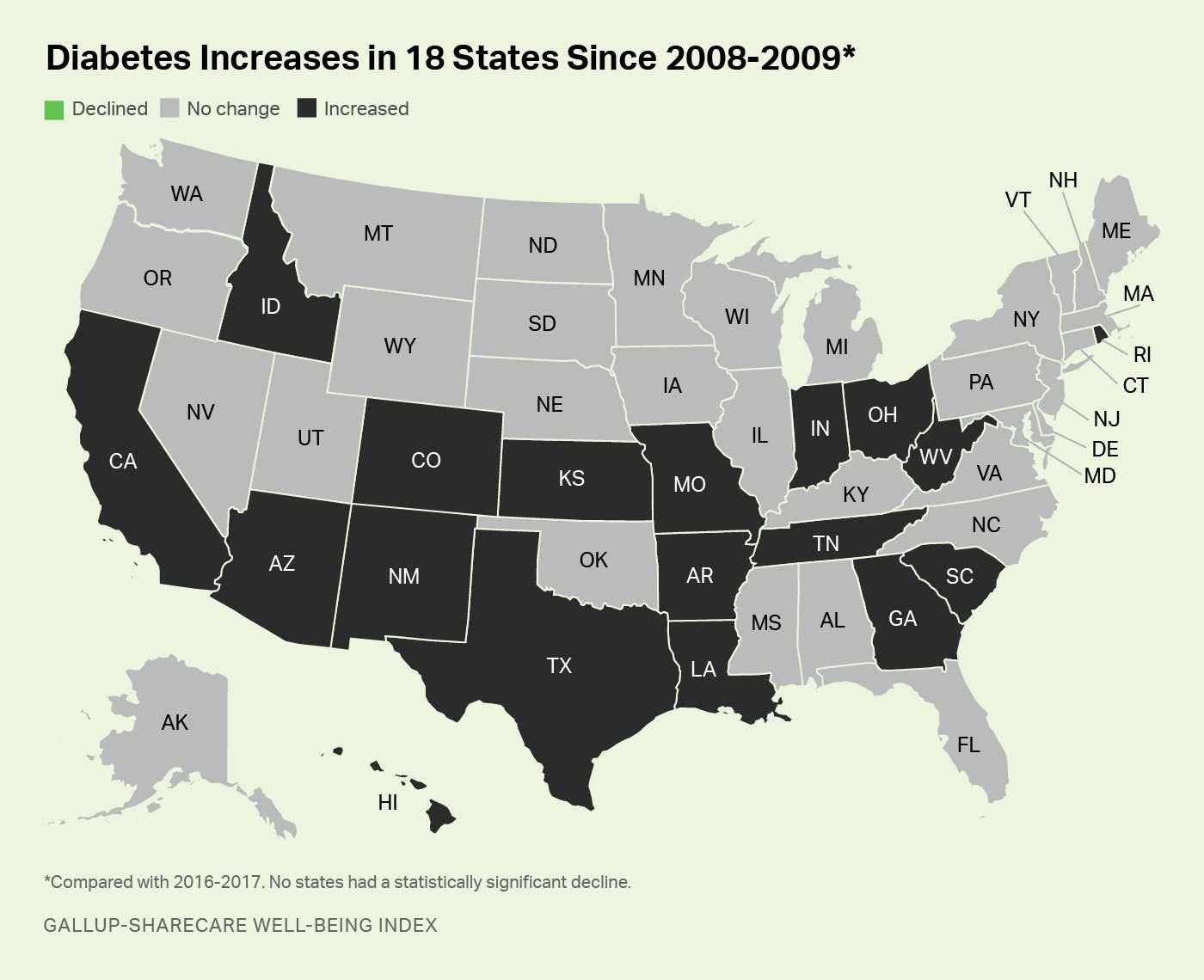
Of the 18 states where the diabetes rate has increased, five have seen an increase of at least two percentage points: West Virginia, Louisiana, Hawaii, Rhode Island and South Carolina. Other states with statistically significant increases are Arizona, Arkansas, California, Colorado, Georgia, Idaho, Indiana, Kansas, Missouri, New Mexico, Ohio, Tennessee and Texas.
Nationally, the diabetes rate reached 11.5% in 2016-2017, up 0.7 percentage points from 10.8% in 2008-2009 and representing net increase of about 1.7 million American adults who report having been diagnosed with the disease during this period.
These data, collected as part of the Gallup-Sharecare Well-Being Indexes, are based on Americans' responses to the question "Has a doctor or nurse ever told you that you have diabetes?" State-level data are based on more than 709,000 daily surveys conducted from January 2008 to December 2009 and more than 337,000 surveys conducted from January 2016 to December 2017. The welfare index does not distinguish between type 1 or type 2 diabetes. [19659010] Alaska and Colorado set the pace for the lowest overall diabetes rate
Although Colorado is one of 18 states that experienced an increase in the percentage of its residents reporting a diagnosis of diabetes, it remains in a nationally rare enterprise as one of six states an overall prevalence of less than 9% in 2016-17. Alaskan residents report the lowest diagnosis rate at 8.4%, while Montana, New Hampshire, Utah and Vermont are the states that exceed this threshold. about twice what was measured among the six lowest states. South Carolina, Mississippi, Kentucky, Louisiana, Arkansas, Alabama and Tennessee are diagnosed with diabetes of at least 14% in 2016-17.
The lowest and highest prevalence of diabetes in 2016-17
Has a doctor or nurse ever told you that you have diabetes? "(% Yes)
| The 10 Lowest States | Diabetes Rate | The 10 Highest States | Diabetes Rate | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | % | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alaska | 8.4 | West Virginia | 17.9 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Colorado | 8.6 | South Carolina | 15.1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Montana | 8.7 | Mississippi | 14.8 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| New Hampshire | 8.8 | Kentucky | 14.4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Utah | 8.9 | Louisiana | 14.4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vermont | 8.9 | Arkansas | 14.2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mbadachusetts | 9.0 | Alabama | 14.1 | 19659025] Minnesota | 9.4 | Tennessee | 14.1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Wyoming | 9.5 | Oklahoma | 13.0 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| From North Dakota | 9.6 | Indiana | 13.0 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ] Results reflect the two-year data collection period from January 2016 to December mbre 2017 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gallup-Sharecare Well-being Index | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
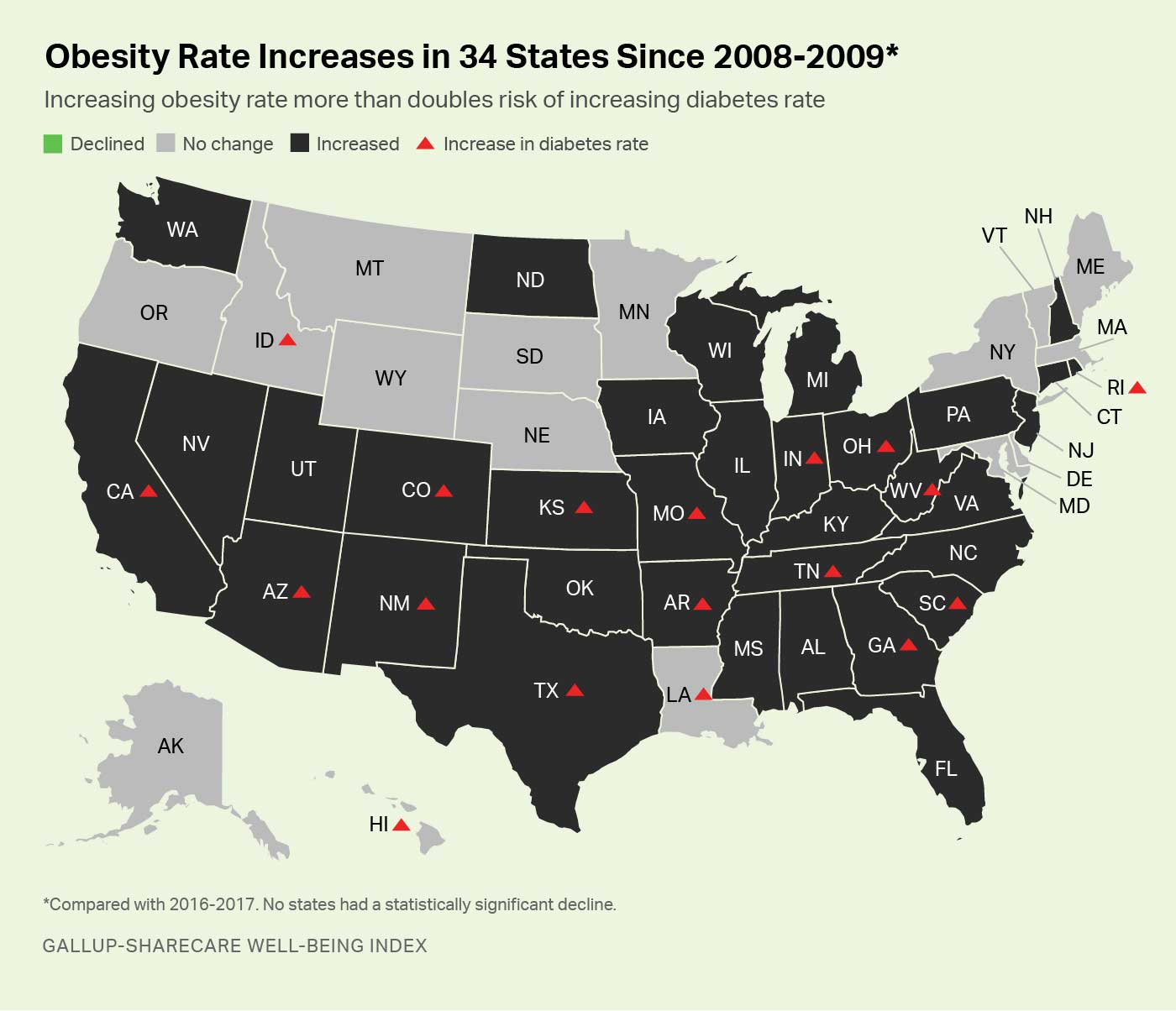
The obesity rate is increasing in 34 states since 2008-2009
A factor like The increase in the prevalence of obesity has also contributed to the increase in the number of diagnoses of diabetes during the last decade. Obesity has been shown to quadruple the risk of diabetes in adults of most age groups, and a rising obesity rate at the state level more than doubles the chances that the state will also experience an increase in diabetes.
Over the two-year period between 2008 and 2009, 26.0% of US adults were obese, based on body mbad index (BMI) calculations based on self-badessments of their height and weight. their weight. This figure reached 28.3% in 2016-2017. This has resulted in an increase in obesity rates in 34 states, while obesity has declined in none. Among states with increased obesity, 15 – or 44% – also had a statistically significant increase in diabetes. In contrast, diabetes increased only in three of the 16 states that had no significant changes in obesity, or 19%. Thus, states with rising obesity rates are about 2.3 times more likely to also experience an increased prevalence of diabetes than states with no increasing obesity rates.
As a general rule, states in areas of high general welfare are more likely to avoid increases. in obesity and diabetes, the states of Northern Plains, Mountain West and Northeast provide most of these examples. South Dakota, Vermont, Minnesota, Montana, Mbadachusetts, Wyoming, Alaska, and Nebraska all have states with the highest scores on their index of well-being, and all have resist the deterioration of national trends in both cases.
Contrary to some government estimates of obesity, the Gallup-Sharecare Well-Being Index uses self-reported height and weight of respondents to calculate BMI and the following weight categories. These are not clinical measures that usually result in higher estimates of obesity. A BMI equal to or greater than 30 gives rise to a clbadification of obesity.
Implications
Diabetes can be caused by many factors. Type 1 diabetes is an autoimmune disease that affects about 5% of the American population. It is at least partially linked to genetics, with possible environmental triggers. Type 2 diabetes, which is much more prevalent, is linked to inactivity, family history, smoking, excessive drinking and high blood pressure. The link between obesity and type 2 diabetes is particularly well understood because of the known relationship between the accumulation of adipose tissue in the body and the resultant insulin-like cell resistance. .
Community and state leaders can take a sensible approach to reducing type. 2 risk factors for diabetes. For example, the many bike paths and well-organized neighborhoods that allow residents to perform routine chores on foot or by bike are proven methods to reduce both obesity and diabetes. Public parks and other green spaces that encourage outdoor travel also have strong inverse relationships between the two conditions.
Local businesses and schools can also be encouraged to do their part. Grocery stores, for example, can promote healthy rather than unhealthy foods by placing fresh products and other healthier options at the front of the grocery store, so that customers are the best. first to choose. Free healthy cooking clbades and recipes for cooking at home are also a useful approach. Restaurants, in turn, can offer healthy options clearly marked on the menu, as well as nutritional information for each menu option so that customers can make informed choices when ordering. And local schools can organize "school buses on foot" and limit unhealthy choices in the cafeteria to help students adopt healthy eating habits. Business leaders can set the agenda at their workplace to optimize better eating habits and reward positive or positive employee health outcomes by contributing to the flexibility of expense accounts and to other tools.
The management of diabetes best practices by health care providers in turn combines educational services, innovative outpatient prevention, and well-organized self-management processes designed to better achieve glycemic goals. And multidisciplinary teams that provide coordinated care are increasingly recognized as clinically effective ways to maximize the quality of life of patients with diabetes.
"Health professionals and policy makers need to work together to create environments that give people the opportunity to choose a healthy lifestyle," says Sheila Holcomb, Vice President, Sharecare. "It's only thanks to this type of encouragement that a behavioral change will affect people with diabetes and prediabetes, and will reduce the prevalence rate and the rising costs badociated with its treatment." "
For a full report on diabetes rates in states and cities across the country, visit https. : //wellbeingindex.sharecare.com.

[ad_2]
Source link
