
[ad_1]
MIT researchers have invented a new type of amputation surgery that can help amputees better control their residual muscles and detect where their “phantom limb” is in space. This restored sense of proprioception should translate into better control of prosthetic limbs, as well as reduced limb pain, the researchers say.
In most amputations, the pairs of muscles that control the affected joints, such as the elbows or ankles, are severed. However, the MIT team found that reconnecting these pairs of muscles, allowing them to maintain their normal push-pull relationship, gives people much better sensory feedback.
“Our study and previous studies show that the better patients can dynamically move their muscles, the more control they will have. The better a person can operate the muscles that move their phantom ankle, for example, the better able they are to use their prostheses, ”says Shriya Srinivasan, postdoc at MIT and lead author of the study.
In a study to appear this week in the Proceedings of the National Academy of Sciences, 15 patients who received this new type of surgery, called myoneural agonist-antagonist interface (MAI), could control their muscles more precisely than patients with traditional amputations. Patients with AMI have also reported feeling more freedom of movement and less pain in their affected limb.
“Using surgical and regenerative techniques that restore the natural muscle movements of agonist-antagonists, our study shows that people with AMI amputation experience a greater range of motion of the phantom joint, reduced pain level. and increased fidelity of the controllability of prosthetic limbs, ”says Hugh Herr, professor of media arts and sciences, head of the Biomechatronics group at the Media Lab and lead author of the article.
Other authors of the article include Samantha Gutierrez-Arango and Erica Israel, senior research support associates at the Media Lab; Ashley Chia-En Teng, undergraduate student at MIT; Hyungeun Song, graduate student of the Harvard-MIT program in health science and technology; Zachary Bailey, former visiting scholar at the Media Lab; Matthew Carty, visiting researcher at the Media Lab; and Lisa Freed, researcher at the Media Lab.
Restore the feeling
Most of the muscles that control limb movement occur in pairs that alternately stretch and contract. An example of these agonist-antagonist pairs is the biceps and triceps. When you bend your elbow, the biceps muscle contracts, causing the triceps to stretch, and this stretch sends sensory information back to the brain.
In a conventional limb amputation, these muscle movements are limited, cutting off this sensory feedback and making it much more difficult for amputees to sense where their prosthetic limbs are in space or to sense the forces applied to those limbs. .
“When one muscle contracts, the other doesn’t have its antagonistic activity, so the brain receives confusing signals,” says Srinivasan, a former member of the Biomechatronics group who now works at MIT’s Koch Institute for Research integrative on cancer. “Even with state-of-the-art prostheses, people visually follow the prosthesis constantly to try to calibrate their brains for where the device is moving.”
A few years ago, the MIT Biomechatronics group invented and scientifically developed in preclinical studies a new amputation technique that maintains the relationships between these pairs of muscles. Instead of cutting each muscle, they connect the two ends of the muscles in such a way that they always communicate dynamically with each other in the residual limb. In a 2017 study on rats, they showed that when animals contracted one muscle in the pair, the other muscle stretched and sent sensory information back to the brain.
Since these preclinical studies, approximately 25 people have undergone AMI surgery at Brigham and Women’s Hospital, performed by Carty, who is also a plastic surgeon at Brigham and Women’s Hospital. In the new PNAS study, researchers measured the accuracy of muscle movements in the ankle and subtalar joints of 15 patients who had AMI amputations below the knee. These patients had two sets of muscles reconnected during their amputation: the muscles that control the ankle and those that control the subtalar joint, which allows the sole of the foot to tilt inward or outward. outside. The study compared these patients to seven people who had traditional below-knee amputations.
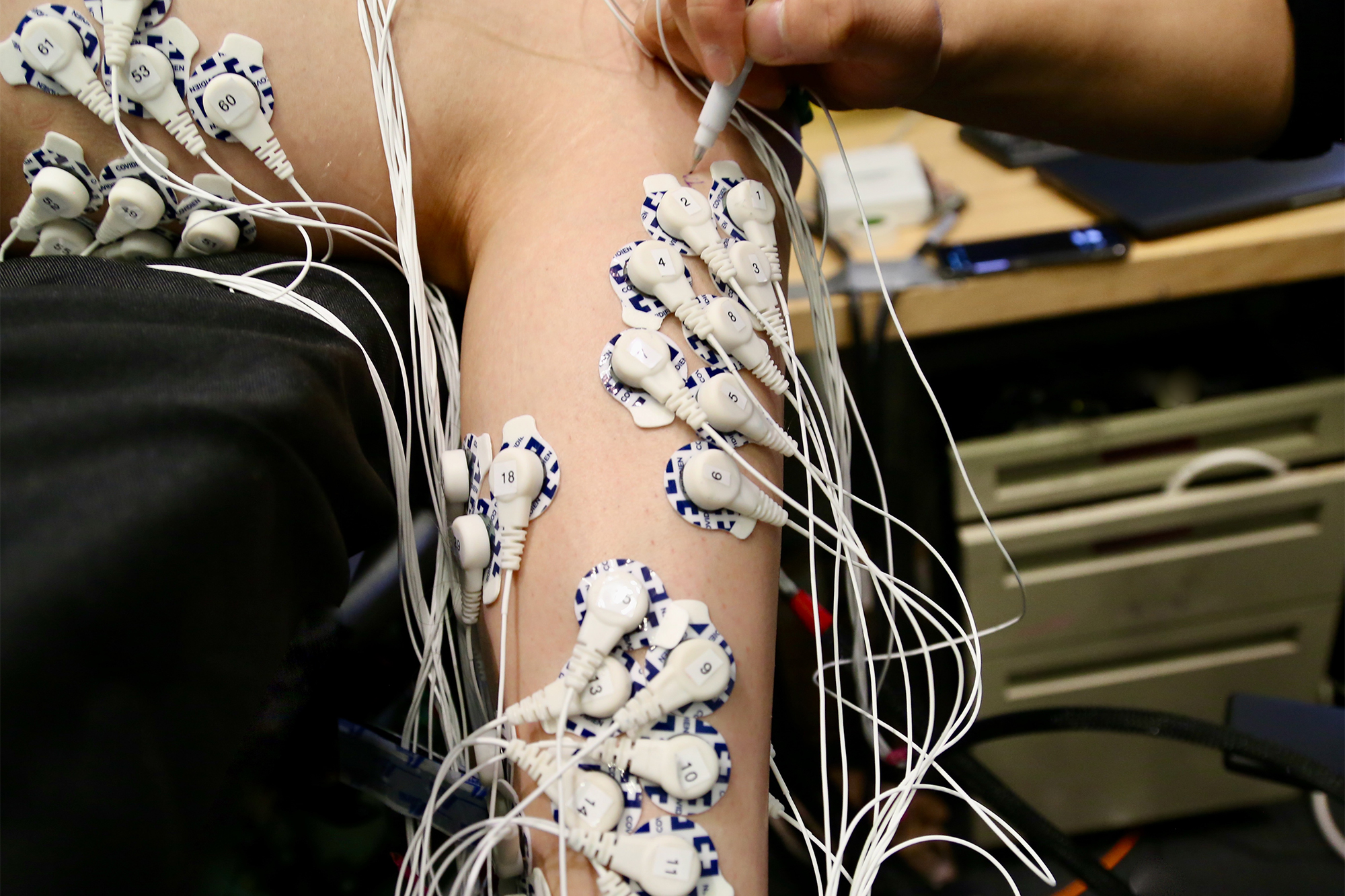
Each patient was assessed in a supine position with their legs supported on a foam pillow, allowing their feet to stretch out in the air. The patients did not wear prostheses during the study. The researchers asked them to flex their ankle joints – both the intact one and the “phantom” – to 25, 50, 75 or 100% of their full range of motion. Electrodes attached to each leg allowed researchers to measure the activity of specific muscles as each movement was repeated.
The researchers compared the electrical signals from the muscles of the amputated limb with those from the intact limb and found that for patients with AMI, they were very similar. They also found that patients with AMI amputation were able to control the muscles of their amputated limb much more precisely than patients with traditional amputation. Patients with traditional amputations were more likely to perform the same movement repeatedly in their amputated limb, regardless of how far they were asked to flex the ankle.
“The ability of AMI patients to control these muscles was much more intuitive than those with typical amputations, which was largely related to how their brains processed phantom limb movement,” Srinivasan explains.
In a recent article in Scientific translational medicine, the researchers reported that brain scans of AMI amputees showed that they received more sensory feedback from their residual muscles than patients with traditional amputations. In work currently underway, researchers are measuring whether this ability translates into better control of a prosthetic leg when walking.
Freedom of movement
The researchers also found an effect they hadn’t anticipated: AMI patients reported significantly less pain and a greater feeling of freedom of movement in their amputated limbs.
“Our study was not specifically designed to accomplish this goal, but it was a sentiment our subjects expressed time and time again. They had a much greater sense of what their foot actually felt and how it moved in space, ”Srinivasan explains. “It became increasingly clear that restoring muscles to their normal physiology had benefits not only for prosthetic control, but also for their day-to-day mental well-being.
The research team has also developed a modified version of the surgery that can be performed on people who have already had a traditional amputation. This process, which they call “regenerative AMI,” involves grafting small muscle segments to serve as agonist and antagonist muscles for an amputated joint. They are also working on the development of the AMI procedure for other types of amputations, including above the knee and above and below the elbow.
“We’re learning that this technique of rewiring the limb, and using spare parts to rebuild that limb, works and is applicable to various parts of the body,” Herr says.
The research was funded by the MIT Media Lab Consortia; National Institute of Child Health and Human Development of the National Institutes of Health and the National Center for Medical Rehabilitation Research; and congressional medical research programs of the US Department of Defense.
[ad_2]
Source link